Andrew Huberman Sleep Protocol for Night Shift Workers: Does It Actually Work?

Andrew Huberman's sleep protocol for night shift workers is a circadian adaptation system built on three tools: light management (blocking morning sunlight after your shift, using bright light at shift start), the temperature minimum (a biological anchor for shifting your alertness window), and a supplement stack of magnesium bisglycinate, apigenin, and L-theanine taken 30–60 minutes before sleep.
Here are the adaptations that work, which ones have limits, and when prescription options become relevant, based on Huberman's research and the clinical evidence on Shift Work Sleep Disorder.
Andrew Huberman's approach sounds reasonable on paper. But if you've actually tried it while clocking a 12-hour night shift, you know it doesn't translate one-to-one. The protocol was designed around a fairly normal circadian rhythm. You don't have one.
That doesn't mean Huberman's science is wrong. A lot of it applies directly to your situation. But some pieces require real adaptation, and a few of them simply cannot overcome what shift work does to the human body.
This guide breaks down each pillar of the protocol, what the research actually shows, how well it works when your "morning" is 7 AM and you've just come home from work, and where you'll need to fill the gaps. If you're also exploring Bryan Johnson's approach, we've put together a companion guide to the Bryan Johnson Blueprint sleep protocol for shift workers.
Key Takeaways
- Night shift work disrupts the body’s natural circadian rhythm, which can make sleep timing, daytime rest, and overnight alertness harder to maintain.
- Light management is one of the most important behavioral tools for shift workers because bright light signals wakefulness, while morning sunlight after a shift can make it harder to fall asleep.
- The temperature minimum concept can help shift workers time light, exercise, and meals in a way that supports circadian adjustment.
- Sleep supplements such as magnesium, apigenin, and L-theanine may help with sleep onset, but they do not fully solve daytime sleep fragmentation caused by light, noise, or schedule disruption.
- Rotating shift workers face a harder challenge than permanent night shift workers because the body usually needs consistency to adapt to a new sleep-wake cycle.
- Behavioral sleep protocols can help, but persistent sleepiness may require a broader evaluation because Shift Work Sleep Disorder is a recognized medical condition with clinical treatment options.

Huberman's Core Framework for Night Shift Workers
Andrew Huberman is a neuroscientist at Stanford who hosts the Huberman Lab podcast. His sleep protocol isn't a single intervention, it's a layered system built around circadian biology. The core principles:
- Light anchors your clock. Morning sunlight (ideally within 30–60 minutes of waking) signals the brain to start the cortisol awakening response and begin the countdown to melatonin release 12–16 hours later.
- Temperature drives sleep transitions. Core body temperature drops as you fall asleep and rises as you wake. Managing this curve is how you shift your sleep timing.
- Supplements support, not replace, good sleep hygiene. His "sleep cocktail" uses magnesium, apigenin, and L-theanine to reduce neural excitability and ease the transition to sleep.
- Non-Sleep Deep Rest (NSDR) recovers lost sleep. Yoga Nidra and similar practices can restore some neurological function even when full sleep isn't possible.
That architecture is scientifically sound. The problem is it assumes your waking hours are daytime. As a night shift worker, your challenge isn't just sleep hygiene, it's that your biology is running in permanent opposition to your schedule.
The Temperature Minimum: Your Most Useful Tool
Of everything Huberman teaches, the temperature minimum concept translates most directly to night shift workers.
Your temperature minimum is the point in every 24-hour cycle when your core body temperature is at its lowest, typically 90 minutes before your natural wake time. Huberman's key insight: what you do in the two hours after your temperature minimum shifts your clock forward or backward.
- Light, exercise, or eating after your temperature minimum advances your clock (makes you want to be awake and alert earlier)
- Doing those things before your temperature minimum delays your clock (pushes wakefulness later)
For a night shift worker whose "natural" body clock might be set to sleep from 6 AM to 2 PM, the temperature minimum falls around 4:30 AM. If you get home at 7 AM and immediately expose yourself to morning sunlight, you're hitting that window and sending your brain a wakefulness signal at exactly the wrong time.
That's why wearing sunglasses on your commute home, then using a sleep mask once you are home and ready to sleep, is one of the most important behavioral interventions you can make as a night shift worker following Huberman's protocol.
Conversely, getting bright, ideally blue-spectrum light at the start of your night shift (9–10 PM) helps push your alertness peak into the hours when you need it most.
The Huberman Lab episode on shift work and jet lag walks through this in detail. It's one of the better practical applications of circadian science for this population.
Light Management: Where Shift Workers Win or Lose
Light management is the single most powerful lever in the Andrew Huberman sleep protocol for night shift workers, more impactful than supplements, NSDR, or temperature adjustments. Light is the primary input your circadian system uses to set its 24-hour clock, which means controlling it correctly can shift your alertness window by hours; getting it wrong undermines everything else.
During your shift:
- Use bright overhead lights or a light therapy box (10,000 lux) during your first few hours at work
- Avoid dim environments in the early part of your shift, they signal your brain that sleep is approaching
- Blue-enriched light at peak sleepiness (often 3–5 AM) has been shown to improve alertness and on-the-job performance, according to research on shift work and sleep
After your shift:
- Wear blue-light-blocking sunglasses during your commute home, then use an eye mask once you are home and ready to sleep. Morning sunlight is extremely powerful and will blunt your ability to fall asleep
- Once home, use blackout curtains, not just "light-blocking" curtains. Total darkness, not 80% darkness
- Keep your phone on do-not-disturb; light from screens within 30 minutes of sleep significantly delays melatonin onset
This is where most night shift workers underinvest. The commute home without eye protection, five minutes on the phone in bed, a baby crying in the next room, these add up. The light management piece of Huberman's protocol is the most evidence-backed, and also the hardest to execute in a real household.
Huberman's Sleep Stack: What the Supplements Actually Do
Huberman's core supplement protocol, taken 30–60 minutes before your target sleep time:
A few honest notes:
What they do well: These supplements reduce the anxious, wired feeling that prevents sleep onset. For shift workers who get into bed at 8 AM still feeling alert from work adrenaline, they can meaningfully shorten how long it takes to fall asleep.
What they don't fix: Daytime sleep is structurally lighter than nighttime sleep. Your brain is fighting light, sound, and a biological clock screaming that it's time to be awake. Supplements reduce arousal at the margins, they can't override a cortisol rhythm that's misaligned with your schedule.
L-theanine caveat: Huberman himself notes that L-theanine can intensify dreams and may worsen sleepwalking or night terrors in some people. If you're already having vivid or disturbing dreams on rotating shifts, start with magnesium and apigenin first, then add L-theanine if needed.
On melatonin: Notably absent from Huberman's stack. He's skeptical of doses that exceed your body's natural production (typically 0.1–0.3 mg), while most OTC melatonin is 5–10 mg. If you use melatonin, timing matters enormously, taken at the wrong phase of your cycle, it can deepen the misalignment rather than correct it.
Where Huberman's Protocol Has Limits
Huberman's protocol was developed for human beings with roughly normal circadian rhythms who want better sleep. For permanent night shift workers who've had years to partially adjust, many elements translate well. For rotating shift workers, especially those alternating every few days, the picture is different.
Protocol effectiveness by shift type:

The rotating shift problem: Your body needs at least two weeks on a consistent schedule to meaningfully shift circadian timing. Rotating every three to five days means you're never adjusting, you're perpetually jet-lagged. Huberman's light and temperature tools still help at the margins, but the biological substrate isn't there to anchor the change.
Sleep environment reality: Blocking light and sound is theoretically straightforward. In practice, if you share a home with people who are awake during the day, it's a significant logistical challenge. Partner, children, and the ambient noise of a house in daylight hours can fragment sleep in ways no supplement fully offsets.
The cumulative debt: About 25–30% of night and rotating shift workers meet criteria for Shift Work Sleep Disorder, according to research published in the journal Sleep Medicine. The average person with SWSD loses one to four hours of sleep per night.
Over weeks and months, that debt compounds. The National Safety Council estimates that 13% of annual workplace injuries are fatigue-related. At that level of accumulated sleep loss, behavioral protocols, including Huberman's, help at the margins, but they rarely close the gap on their own.
NSDR and Sleep Recovery Tools
Non-Sleep Deep Rest (NSDR) is the most underrated tool in Huberman's entire protocol for night shift workers, and the one most people skip. The protocol involves guided deep relaxation that slows brainwave activity without requiring full sleep, making it uniquely practical for people who can't schedule an uninterrupted 7-hour block.
Studies on Yoga Nidra, the primary NSDR practice Huberman recommends, suggest that 10–20 minutes can improve cognitive function, reduce stress markers, and help restore neurological function lost during abbreviated sleep. For shift workers who can't get a full sleep block, an NSDR session before a shift or during a break is worth building into your routine.
Huberman recommends finding free Yoga Nidra recordings on YouTube, 10 minutes is enough for measurable benefit on alertness and mood. Based on our analysis, NSDR is the highest-return Huberman tool for shift workers relative to the effort required: zero equipment, zero cost, and measurable recovery in under 20 minutes.
Other practical recovery tools that pair well with the protocol:
- Short naps (10–20 min): Research supports napping before night shifts to reduce sleepiness during the shift. Avoid naps longer than 30 minutes during your scheduled sleep window, as they fragment the main block.
- Caffeine timing: Huberman suggests waiting 90–120 minutes after waking before consuming caffeine to allow adenosine to clear naturally. For night shift workers, this means not reaching for coffee the moment you wake up before your shift.
- Consistent meal timing: Eating within a restricted window (8–10 hours) helps anchor metabolic rhythms that support circadian health, even when sleep timing is irregular.
When Behavioral Tools Aren't Enough: SWSD Options
For most people, Huberman's protocol will improve sleep quality at the margins. For a meaningful segment of night shift workers, it won't be sufficient, and that's not a failure of discipline. SWSD is a recognized medical condition, and it has recognized medical treatments.
Modafinil and SWSD: Modafinil, a wakefulness-promoting agent, was FDA-approved specifically for excessive sleepiness associated with Shift Work Sleep Disorder in 2004. In a landmark New England Journal of Medicine trial, 209 patients with SWSD received 200 mg of modafinil or a placebo before each shift. The result: 74% of modafinil-treated patients showed clinical improvement, compared to 36% for placebo.
Crucially, modafinil works through mechanisms different from stimulants like Adderall. It promotes wakefulness without triggering the cardiovascular side effects or abuse potential associated with Schedule II medications. Modafinil is classified Schedule IV, lower risk profile, meaningful clinical impact.
How MOD fits here: MOD Alert is a prescription medication containing 150 mg modafinil plus 60 mg caffeine, designed specifically for shift workers managing SWSD. It's not an over-the-counter supplement or an energy drink, it's a compounded medication prescribed through a telehealth provider. The process: complete an online assessment, a licensed provider reviews your information, and if appropriate, MOD ships directly to you. No waiting rooms.
MOD Alert isn't a replacement for the behavioral strategies above. It works alongside them. The best outcomes for SWSD combine circadian hygiene (Huberman's tools) with appropriate medical support when chronic sleepiness persists.
Final Verdict
Huberman's protocol isn't a silver bullet for night shift workers, but it's the most evidence-backed set of behavioral tools available, and the parts that work, work well.
Here's how to apply it based on your situation:
- Permanent night shift workers: Follow the adapted protocol fully. Light management (blocking morning sun, using bright light at shift start) and temperature minimum timing can produce measurable results over 2–4 weeks on a consistent schedule.
- Rotating shift workers: Prioritize light management and blocking morning sun exposure. True circadian adaptation isn't possible on a 3–5 day rotation, but aggressive light control limits the damage.
- Anyone with persistent sleepiness despite good sleep hygiene: This is the gap behavioral protocols can't fully close. SWSD is a recognized medical condition. If you've applied light management, supplements, and NSDR consistently for 4+ weeks and still struggle, it's worth talking to a provider about whether prescription support makes sense.
If that last point describes you, MOD Alert, a medication containing 150 mg modafinil plus 60 mg caffeine, was designed specifically for shift workers with SWSD. It's prescribed through a telehealth intake and ships to your door.

Frequently Asked Questions
Does Andrew Huberman's sleep protocol work for night shift workers?
It works partially. The core tools, light management, temperature minimum timing, and sleep supplements, are grounded in solid circadian biology and apply to shift workers. The protocol works best for permanent night shift workers who can establish a consistent schedule. It's less effective for rotating shift workers whose bodies never stabilize on a single cycle.
What is the Huberman sleep supplement stack?
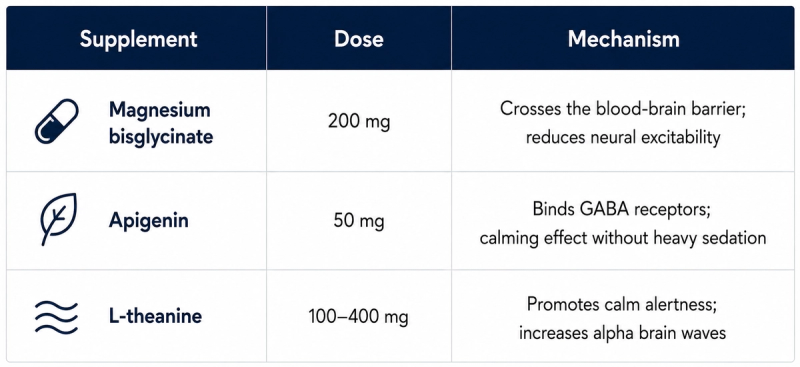
Huberman's core sleep stack is magnesium bisglycinate (200 mg), apigenin (50 mg), and L-theanine (100–400 mg), taken 30–60 minutes before sleep. He does not recommend standard over-the-counter melatonin doses (5–10 mg), preferring lower doses (0.1–0.3 mg) if melatonin is used at all. The stack reduces neural excitability and eases the transition to sleep, useful for shift workers who feel wired after a night shift.
What is Shift Work Sleep Disorder (SWSD)?
SWSD is a circadian rhythm sleep disorder affecting people whose work hours overlap with their body's natural sleep period. It's characterized by excessive sleepiness, insomnia, or both. Research estimates it affects approximately 25–30% of night and rotating shift workers. The condition is associated with elevated risks of cardiovascular disease, metabolic disorders, cognitive impairment, and workplace accidents.
Is modafinil safe for night shift workers?
Modafinil is FDA-approved for excessive sleepiness associated with SWSD and has a well-studied safety profile in this population. It's classified as Schedule IV (lower abuse potential than Schedule II stimulants like Adderall). Common side effects include headache (21%) and nausea (12%), per the landmark SWSD clinical trial. It's important to discuss your full medical history with a provider before starting any prescription medication.
How do I reset my circadian rhythm on rotating shifts?
True circadian reset on rotating shifts is difficult because your schedule changes faster than your body can adapt (adaptation takes roughly two weeks). The best approach: use light management aggressively (bright light when you need to be awake, total darkness when sleeping), time exercise and meals consistently relative to your shift start, and minimize light exposure during your commute home. If possible, advocate for consistent shift schedules with your employer, research strongly supports staying on one shift for at least two weeks at a time.
What Is the Temperature Minimum for Shift Workers?
Your temperature minimum is the point in every 24-hour cycle when your body temperature is lowest, typically 90 minutes before your natural wake time. Exposure to light, exercise, or food in the two hours after your temperature minimum advances your clock (shifts wakefulness earlier). Doing those things before your minimum delays it (pushes wakefulness later). Shift workers can use this principle to intentionally shift their alertness windows, and to understand why morning sunlight exposure after a night shift actively sabotages their ability to sleep.
What Shift Worker Mistakes Undermine Huberman's Protocol?
The biggest one is treating it as an all-or-nothing system and giving up when one piece doesn't work. The most frequent specific mistakes: not blocking morning sunlight on the commute home (this single habit undermines everything else), using standard 5–10 mg melatonin doses at the wrong time, and skipping NSDR because it feels too passive. The second most common mistake is expecting results in days, circadian adaptation takes two to three weeks of consistency.
Can I Use Huberman's Protocol With SWSD Medications?
Yes. These approaches are complementary. Huberman's behavioral tools address the root causes of circadian misalignment, prescription medications like modafinil address the wakefulness deficit that remains even with good sleep hygiene. For people with clinically significant SWSD, combining both tends to produce better outcomes than either alone.
Does melatonin help night shift workers sleep?
Melatonin can help night shift workers sleep when timed correctly, but timing matters more than dose. Huberman recommends very low doses (0.1–0.3 mg) if used at all, standard OTC melatonin (5–10 mg) can cause downstream hormonal effects and may deepen circadian misalignment when taken at the wrong phase. For shift workers, a low-dose melatonin taken immediately before your target sleep window is more effective than using it as a general sleep aid.
What is the best sleep schedule for night shift workers?
The best sleep schedule for night shift workers is one that stays consistent, including on days off. Research supports sleeping in one 7–8 hour block immediately after your shift ends, with complete darkness and noise control. If a single block isn't possible, a split schedule (4–5 hours after the shift plus a 1–2 hour nap before the next shift) performs well, provided the anchor sleep period remains consistent from day to day.
How long does it take to adjust to working night shifts?
Full circadian adaptation to night shift work takes approximately six to twelve weeks on a consistent schedule. The biological clock shifts gradually, roughly one to two hours per day under ideal conditions with aggressive light management. Rotating shift workers who change schedules more frequently than every two weeks cannot achieve full adaptation; their bodies are perpetually in transition without establishing a stable anchor point.
This article is provided for informational purposes only and does not constitute medical advice. The information presented is not a substitute for professional medical advice, diagnosis, or treatment. Always consult your healthcare provider to discuss the risks, benefits, and appropriateness of any treatment.
MOD offers access to healthcare providers who may prescribe compounded medications for the treatment of excessive daytime sleepiness associated with shift work sleep disorder (SWSD), when clinically appropriate.
The featured products include compounded medications that have not been approved by the FDA. Compounded medications may be prescribed under federal law but are not the same as, nor are they generic versions of, any FDA-approved medication. The FDA does not review compounded medications for safety, effectiveness, or manufacturing quality of compounded products. A prescription will only be written if deemed appropriate after the digital consultation by the licensed medical provider. Individual results may vary.