How to Get Diagnosed With Shift Work Sleep Disorder in 2026
How to get diagnosed with shift work sleep disorder in 2026 starts with a clinician matching insomnia or excessive sleepiness to a nontraditional schedule, reviewing sleep timing evidence, and ruling out lookalikes such as sleep apnea or narcolepsy. Shift work sleep disorder is a circadian rhythm sleep-wake disorder, so the diagnosis is a timing diagnosis, not just a fatigue complaint.
Sleep Foundation notes that people with SWSD often lose 1 to 4 hours of sleep per night. It also estimates that as many as 20% of shift workers in industrialized countries may meet the condition. In a 2016 CDC/NIOSH national sample, 61.8 percent of night-shift workers reported short sleep duration versus 35.9% of daytime workers. That historical gap helps explain why the diagnostic history matters so much.
This guide covers what counts toward a diagnosis, how to prepare, which tests may come up, and what usually happens after SWSD is confirmed.
Key Takeaways
- SWSD diagnosis is based on symptom timing plus ruled-out alternatives, not just feeling tired during night shifts.
- Clinicians look for insomnia during your intended sleep time, excessive sleepiness at work, or both, tied to a nontraditional schedule for at least 3 months.
- A 14-day sleep log is one of the most useful tools you can bring to the visit.
- Actigraphy can add objective data when your clinician wants to see your sleep-wake pattern across workdays and days off.
- A sleep study is usually ordered to rule out another disorder, such as sleep apnea, not to prove SWSD by itself, according to NCBI StatPearls.
- If you are diagnosed, next steps can include schedule changes, light management, sleep-specific treatment, and a medication discussion when appropriate.

Before You Start
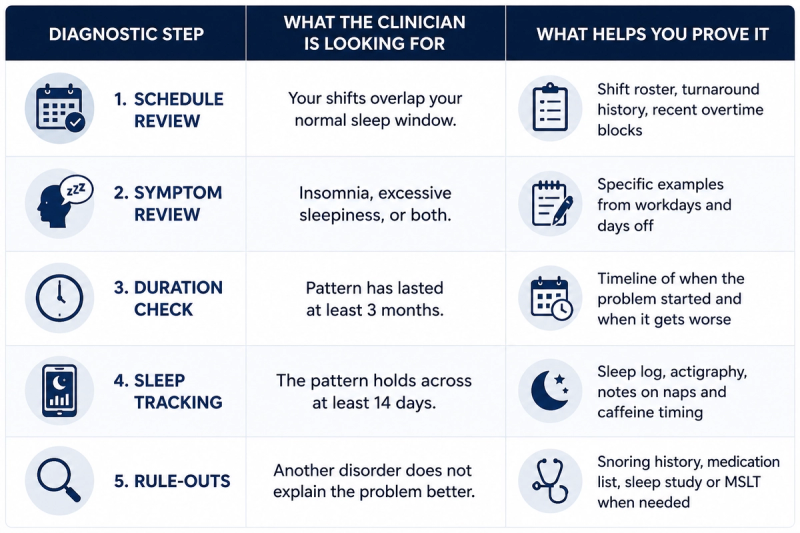
Before you book the visit, know what a real SWSD workup includes. If you are trying to understand how to get diagnosed with shift work sleep disorder, your clinician is looking for a shift-linked pattern, not just a general complaint about being tired. The diagnostic standard summarized by Sleep Foundation and this StatPearls review is consistent:
- Your work hours overlap your normal biological sleep time.
- You have insomnia during your intended sleep time, excessive sleepiness while awake, or both.
- The pattern has been present for at least 3 months.
- Sleep logs or actigraphy show a disrupted pattern over at least 14 days.
- Another sleep disorder, medical issue, medication effect, substance, or poor sleep hygiene does not explain the whole picture better.
It helps to gather three things before the appointment:
- Your shift roster or recent work schedule
- A 14-day sleep log
- A short symptom summary with examples of sleepiness, insomnia, or safety issues
Step-by-Step Instructions
Diagnosis usually comes from matching shift-linked insomnia or sleepiness to your schedule, reviewing a 14-day sleep record, and ruling out better explanations. Those better explanations often include sleep apnea or narcolepsy.
Step 1: Describe the schedule problem clearly
Tell your clinician exactly when you work, how often shifts rotate, and whether symptoms are worse on nights, early mornings, or turnaround shifts. If your sleep gets worse only when your schedule flips, say that directly.
Step 2: Show which symptoms count
SWSD usually shows up as insomnia when you try to sleep, excessive sleepiness when you are trying to stay alert, or both, according to Sleep Foundation.
That often looks like:
- You lie awake after getting home from a night shift even when you are exhausted.
- You wake too early and cannot get back to sleep.
- You fight sleep at work, while charting, while driving home, or during quiet tasks.
- You sleep longer on days off but still feel unrefreshed.
- You are making more near-mistakes or missing turns on the drive home.
Step 3: Show duration, not just severity
Clinicians generally want to see the problem tied to your shift schedule for at least 3 months. A one-week rough patch after overtime is not the same thing as a stable disorder pattern.
Step 4: Bring a 14-day record
A sleep log and actigraphy can help prove the pattern is consistent. Your log should track:
- Shift start and end times
- Bedtime and estimated sleep onset
- Wake time
- Total sleep time
- Naps
- Caffeine timing
- Alcohol or sleep-medication use
- Commute near-misses or on-shift microsleeps
Pair the log with your actual rota or a screenshot of your upcoming shifts. That makes the visit faster and more useful.
Step 5: Rule out lookalikes
Sleep apnea, narcolepsy, medication side effects, alcohol, cannabis, and basic sleep deprivation can mimic parts of SWSD. Doctors usually start with sleep history, a 14-day log, and sometimes actigraphy, then add targeted testing only when another disorder seems likely.
What To Bring to the Appointment
Bring a short, specific packet with your shift roster, 14-day sleep log, and a one-page symptom summary your clinician can scan quickly. For most people, how to get diagnosed with shift work sleep disorder comes down to how clearly they document timing and impairment.
Use this appointment checklist:
- A 14-day sleep log
- Your shift roster or rotating schedule
- A list of current medications
- Caffeine timing and amount
- Alcohol, nicotine, or cannabis use
- Notes on snoring, witnessed breathing pauses, or leg jerks
- Any recent near-miss accident or commute safety event
- Questions about work notes, accommodations, or treatment options
NCBI StatPearls says clinicians should obtain a detailed history of sleep-wake patterns on both working and non-working days. That history should also cover excessive sleepiness, accident risk, other sleep disorders, and medication or substance use.
Tips for Best Results
If you want a cleaner answer faster, these habits help:
- Fill out the full 14-day log before the visit instead of trying to remember details in the room.
- Track caffeine timing honestly, especially if you are relying on coffee, pills, or energy drinks to stay functional.
- Note whether symptoms improve on days off or only after several nights away from shift work.
- Bring questions about work notes, accommodations, and what kind of follow-up testing might happen.
- If treatment comes up later, it’s important to ask about timing, potential side effects, and whether a telehealth prescription is appropriate for your situation.
What Tests Help Rule Out Lookalikes?
Sleep Foundation says many patients are diagnosed based on sleep history, a 14-day log, and sometimes actigraphy. If actigraphy is used, it is usually worn day and night for 14 consecutive days. How to get diagnosed with shift work sleep disorder is usually more about pattern evidence than one definitive machine-based test.
Additional testing comes in when the story is less clean:
- Polysomnography: a formal sleep study, often used to look for obstructive sleep apnea or another sleep disorder.
- Multiple Sleep Latency Test (MSLT): a daytime nap test that measures how quickly you fall asleep when narcolepsy or unexplained pathological sleepiness is suspected.
Sleep Foundation explains that the MSLT usually consists of four to five naps with two-hour breaks. This review adds that polysomnography is not usually necessary for diagnosing SWSD. It is mainly used when the clinician suspects obstructive sleep apnea or another sleep disorder.
If your symptoms line up neatly with shift work and your sleep log supports it, your clinician often does not need a larger workup.
Can a home sleep apnea test be enough?
Yes, a home sleep apnea test can be enough when snoring or witnessed apneas make obstructive sleep apnea the leading alternative diagnosis. Your clinician may still prefer a lab study if the symptoms are mixed or the first test is inconclusive.
When is an MSLT worth the extra step?
An MSLT is worth the extra step when narcolepsy or unexplained pathological sleepiness remains a serious possibility after the basic workup. It adds value when the diagnosis is genuinely uncertain, not when the history already points clearly to SWSD.

Shift Work Sleep Disorder vs. Insomnia vs. Sleep Apnea
Timing is the key difference: SWSD is tied to work hours that clash with your normal sleep window, while insomnia and sleep apnea can persist regardless of shift pattern.
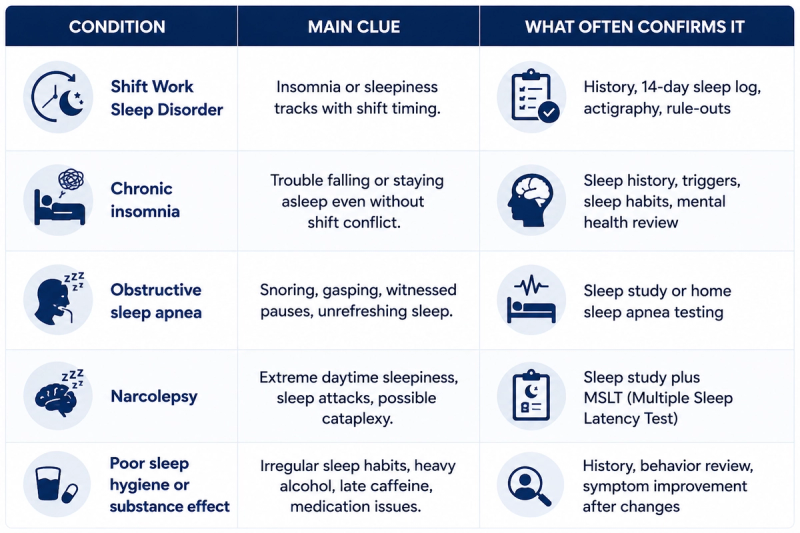
Sleep Foundation says symptoms must not be better explained by another sleep disorder, a medical condition, medication side effects, substance use, or poor sleep hygiene. That is why loud snoring, stimulant use, sedating antihistamines, or untreated anxiety can change the plan.
Common Mistakes That Slow Down an SWSD Diagnosis
Many people slow down the diagnostic process by showing up with fatigue but no pattern. A clinician can work with an imperfect schedule, but a documented symptom timeline is the most useful proof that shift timing is the real driver.
These are the mistakes that create diagnostic fog:
- No sleep log. Without a 14-day record, the clinician has to guess whether your symptoms truly map to your shifts.
- No schedule detail. “I work weird hours” is not enough. Bring exact start times, rotations, and recent changes.
- Forgetting caffeine and medication timing. Late caffeine, over-the-counter sleep aids, or ADHD medication can change how your symptoms are interpreted.
- Ignoring snoring or breathing pauses. If those signs are present, the clinician often rules out sleep apnea first.
- Waiting until a safety incident happens. If you are dozing while charting or nearly falling asleep on the drive home, document it now.
People also normalize the problem for years. You do not want your first hard data point to be a crash or disciplinary event.
When To Talk to Your Doctor
Book the visit sooner rather than later if safety is already becoming a problem. It is also worth escalating care when basic sleep-hygiene changes are not touching the issue.
See a clinician or sleep specialist when:
- You have severe daytime sleepiness despite enough time in bed
- Possible sleep apnea, narcolepsy, or another overlapping disorder is part of the picture
- You are dozing while driving home or having near-miss incidents at work
- Your primary care clinician wants formal testing
- You work in a safety-sensitive role and need clearer documentation
Ask for a medication review if you are relying on escalating caffeine, alcohol to force sleep, or sedating medications after every shift. Those patterns can hide or worsen the disorder.
What Happens After an SWSD Diagnosis
After diagnosis, treatment usually starts with schedule protection, light management, sleep planning, and medication discussion when symptoms remain severe or safety-sensitive:
- Protecting a stable post-shift sleep window
- Using darkness after work and bright light at the right time
- Cutting caffeine early enough to preserve daytime sleep
- Treating coexisting problems such as sleep apnea or chronic insomnia
If symptoms are still strong after that, medication often enters the discussion. Consult your healthcare provider before starting medication or changing timing. DailyMed states that modafinil, a wakefulness-promoting agent, is indicated to improve wakefulness in adults with excessive sleepiness associated with shift work disorder. It is typically taken about one hour before the work shift. Potential side effects can include headache, nausea, nervousness, and insomnia, so it’s important to talk with your healthcare provider if they show up or worsen. In a 2005 PubMed trial summary, patients on modafinil were more likely to show clinical improvement than those on placebo.
If you want to explore a telehealth prescription after the diagnostic workup, MOD focuses specifically on shift workers. MOD offers provider-reviewed prescription treatment for shift workers when appropriate. MOD products are compounded medications, not FDA-approved products, even though modafinil as an active ingredient is FDA-approved for SWSD. MOD’s approach centers on prescription-strength, compounded medications for shift workers rather than generic wellness products.
A work note or accommodation conversation often makes sense when you have repeated near-misses, trouble with rotating turnarounds, or clear evidence that certain schedules trigger symptoms. Formal diagnosis can also help make treatment conversations more specific.
If you want a practical next step after diagnosis, explore MOD plans to learn more about provider-reviewed prescription options for shift workers.
Final Thoughts
Getting diagnosed with shift work sleep disorder is not about proving you are tired. It is about showing a consistent pattern: your work schedule overlaps your normal sleep window, your sleep or alertness suffers, and other explanations do not fit better. A 14-day sleep log, shift roster, symptom timeline, and medication list can make that conversation much clearer.
For shift workers who are diagnosed and still struggle after sleep scheduling, light management, and lifestyle changes, MOD may be a practical option to discuss. MOD focuses on compounded prescription medications for people with Shift Work Sleep Disorder, with provider review used to determine whether treatment is appropriate. The goal is not to replace a proper diagnosis, but to give diagnosed shift workers a focused prescription path when wakefulness support is clinically appropriate.

Frequently Asked Questions
How long does diagnosis take?
Diagnosis can often happen in one visit when your symptoms, shift schedule, and 14-day sleep log clearly line up. If your clinician suspects sleep apnea, narcolepsy, medication effects, or another condition, the process may take longer because additional testing may be needed before SWSD can be confirmed.
What does a shift work disorder diagnosis require?
A shift work disorder diagnosis usually requires shift-linked insomnia or sleepiness, a pattern lasting at least three months, and evidence that another condition does not explain the symptoms better. Clinicians often review workdays and days off because SWSD is about timing, not just general fatigue.
What tests are used to diagnose shift work disorder?
Doctors usually use sleep history, a 14-day sleep log, and sometimes actigraphy. A sleep study or MSLT may be added when the clinician suspects sleep apnea, narcolepsy, or another disorder beyond SWSD. These tests usually help rule out lookalikes rather than prove SWSD by themselves.
Can primary care diagnose SWSD first?
Yes. Primary care can often start the diagnosis by reviewing your schedule, symptoms, sleep log, medications, and safety concerns. A referral to a sleep specialist may follow if symptoms are severe, testing is needed, or another sleep disorder may be involved.
Do I need a formal diagnosis before modafinil?
Usually yes, because a formal diagnosis makes prescribing and treatment decisions clearer. DailyMed lists modafinil as indicated to improve wakefulness in adults with excessive sleepiness associated with shift work disorder, so diagnosis matters before medication discussions.
This article is provided for informational purposes only and does not constitute medical advice. The information presented is not a substitute for professional medical advice, diagnosis, or treatment. Always consult your healthcare provider to discuss the risks, benefits, and appropriateness of any treatment.
MOD offers access to healthcare providers who may prescribe compounded medications for the treatment of excessive daytime sleepiness associated with shift work sleep disorder (SWSD), when clinically appropriate.
The featured products include compounded medications that have not been approved by the FDA. Compounded medications may be prescribed under federal law but are not the same as, nor are they generic versions of, any FDA-approved medication. The FDA does not review compounded medications for safety, effectiveness, or manufacturing quality of compounded products. A prescription will only be written if deemed appropriate after the digital consultation by the licensed medical provider. Individual results may vary.